57 Y/M came to casuality with complaints of gemeralized weakness for 1 month, fever for 1 week and altered semsorium for for 3 days
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
CHEIF COMPLAINTS
57 Y/M came to casuality with complaints of gemeralized weakness for 1 month, fever for 1 week and altered semsorium for for 3 days
Patient was apparently alright for the past 1 month since then he has been complaining of generalised weakness. Since 15 days he has been feeling cold even in hot weather and has been switching off all the fans in the house.
He has been suffering with constipation since 10 days. Has not passed stools at all(confirmed by the attender) He did not take any medication for it
He also complained of abdominal distension/bloating due to not passing stools.
Since 1 week he has fever insidious in onset gradually progressive, high grade. Associated with body pains.Not Associated with chills and rigor. Not relieved with medication.Not associated with nausea, vomiting, burning micturition, headache.
Since 3 days -he fell in the washroom two times(on 22/5/1023)and was not able to get up. When his family members found him, he had slurring of speech and altered sensorium.They took him to the Nalgonda government hospital.
There they gave him an enema and his constipation and bloating was relieved immediately.
They also treated him symptomatically. But he was still in altered sensorium and did not cover
They then shifted him to a private hospital as they had contacts there. There they did MRI and found that infarct in the cortical and subcortical regions of occiput.
but due to too expensive in that hospital so after tracheostomy in view of low GCS (24/05/23 morning) they came to our hospital. On the way in the ambulance, he was able to recognise his family. They brought him to the casualty .

Past history
In 2019 end of the year- He has felt "weak" . One fine day he fell down(due to low energy) while cycling and was immediately rushed to the hospital. They told him his cervical nerves got compressed and said he needed surgery. But due to family issues, he didn't get surgery then, and got it done after 2 months( cervical spondylosis surgery). He recovered after 6 months and started walking with support of a stick since then. The doctors then discovered he had problems in the lumbar region as well (4 years back) and needed surgery too, but didn't give consent for that surgery as they told him he would never be able to walk.
H/o htn since 4 years using medication irregularly
N/k/c/ DM, asthma, epilepsy, thyroid, CAD
Personal history:
Diet-mixed
Appetite - normal
Sleep - adequate
Bowel and bladder - bowel (constipation),bladder normal.
Addiction - drinks toddy occasionally
General Examination:
Patient is C/C/C
Moderately build and nourished.




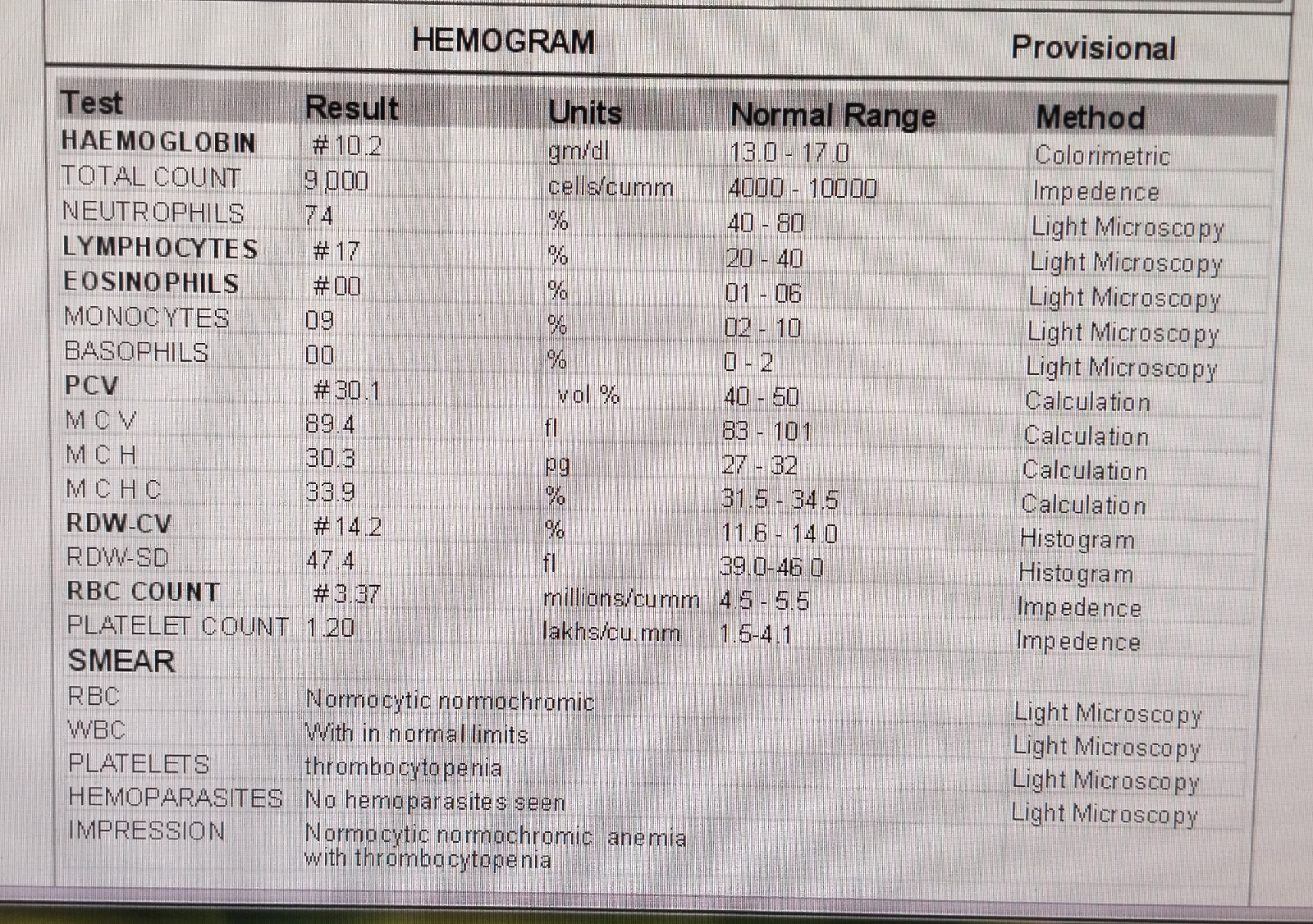
No pallor,icterus,cynosis,clubbing, lymphadenopathy,pedal edema.
Vitals
Temp 101F
Bp -130/90 mmhg
Pr -102 bpm
Rr - 20 cpm
Spo2 100% on 4 liters of RA
Systemic examination:
CNS:
GCS- E4 V (NT) M6
Power -
Rt. Lt
UL - 4/5 4/5
LL - 3/5 3/5
TONE
TONE
UL - N. N
LL - N. N
Reflexes
B - 2+. 2+
T - 2+. 2+
S- 2+. 2+
K - 2+. 2+
A - 2+ 2+
Plantar - extension of big toe in both limbs
RS-B/L air entry present
NVBS
CVS- S1s2present, no murmurs heard
PA- soft and non tender.
PROVISIONAL DIAGNOSIS:
CVA with Acute ischemic stroke (infarct in right occipital lobe ) with Hyponatremia (resolved) with AKI on CKD (resolved) with k/c/o HTN since 3 yrs.
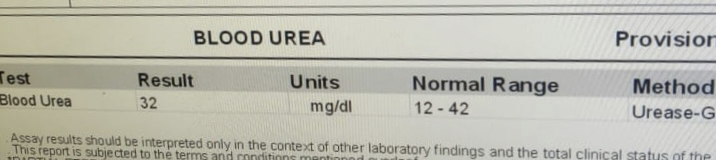
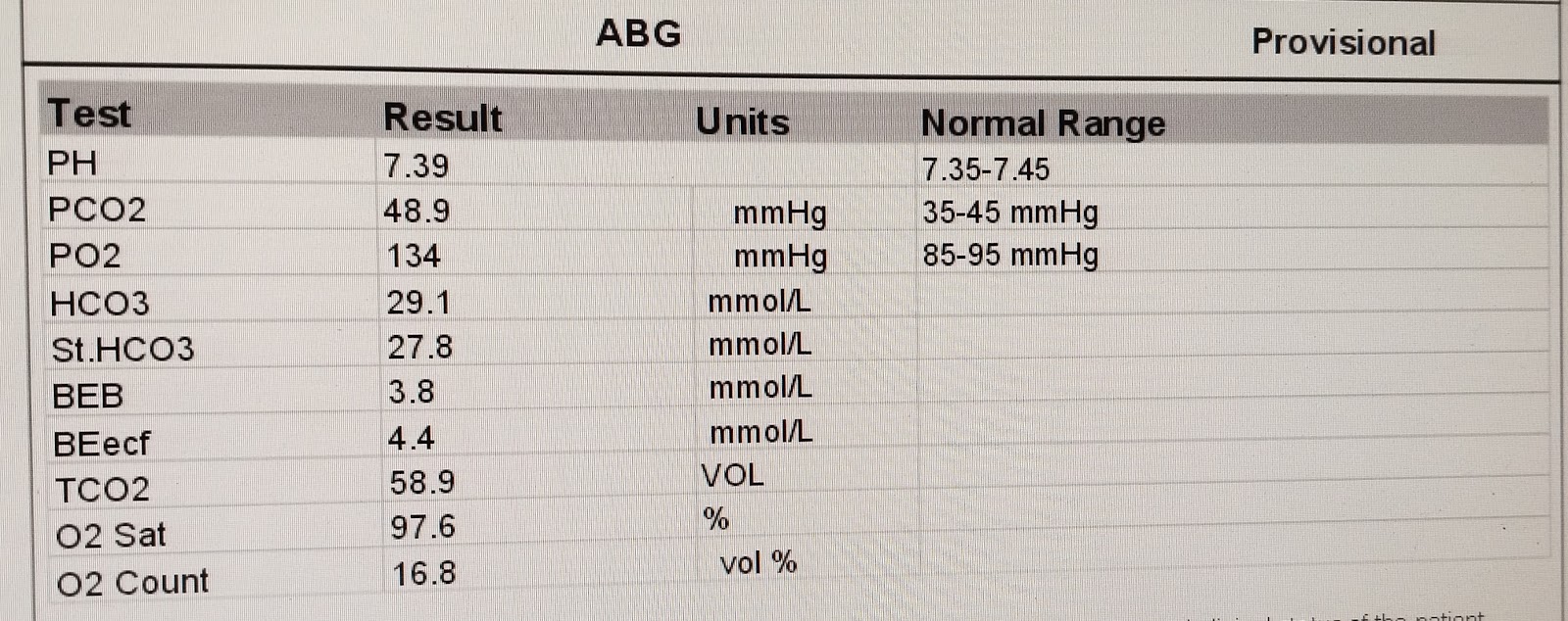
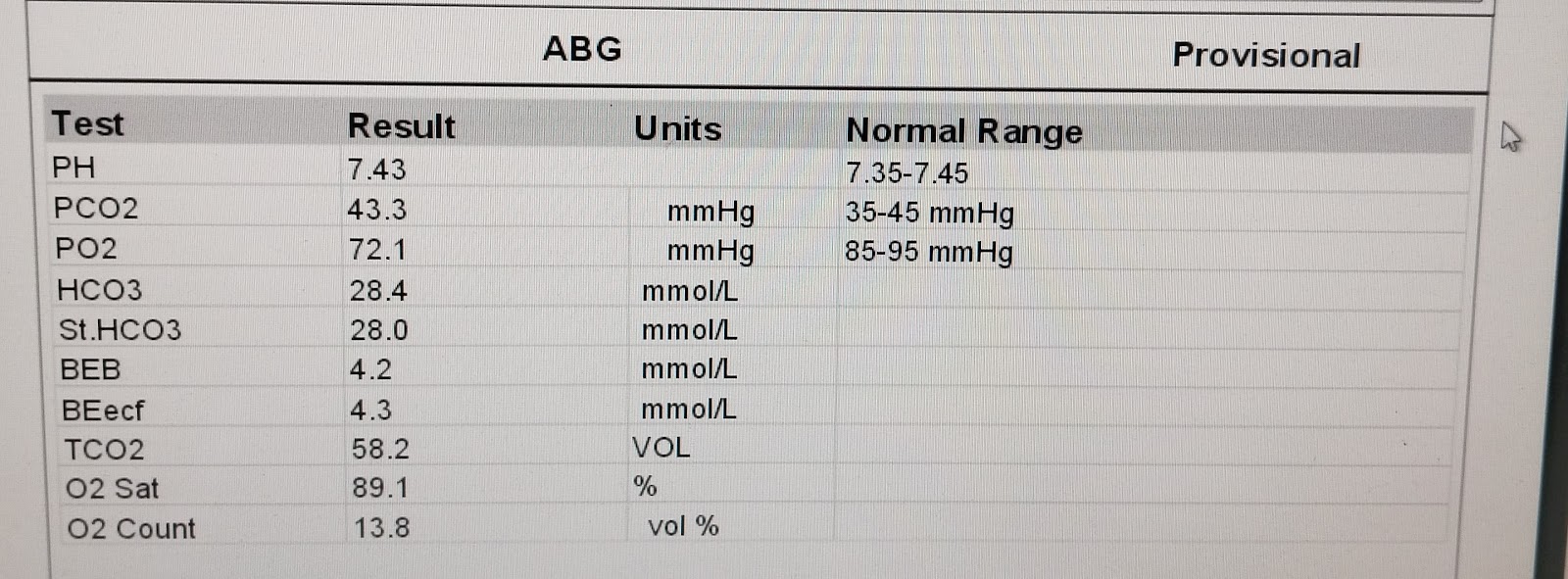
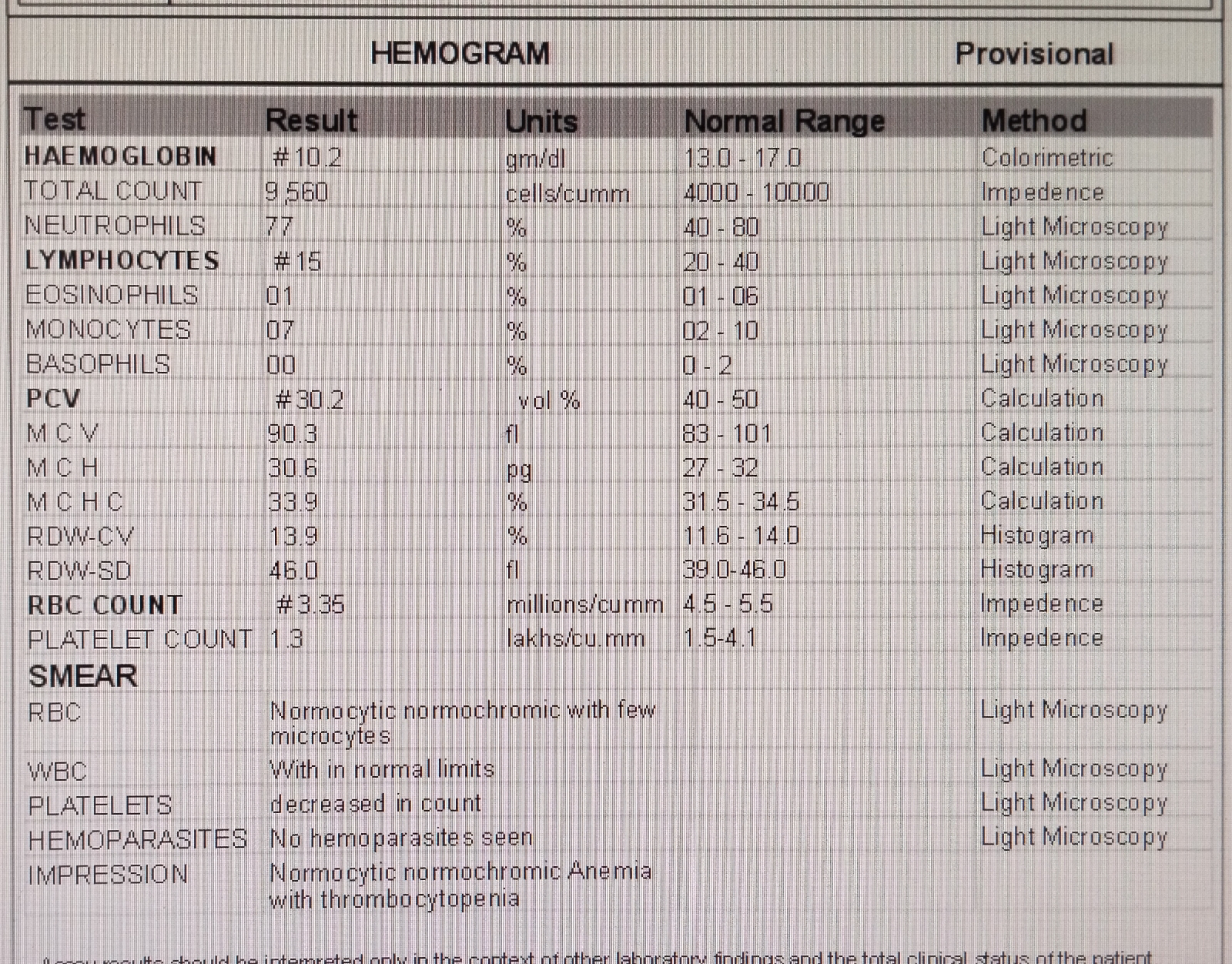
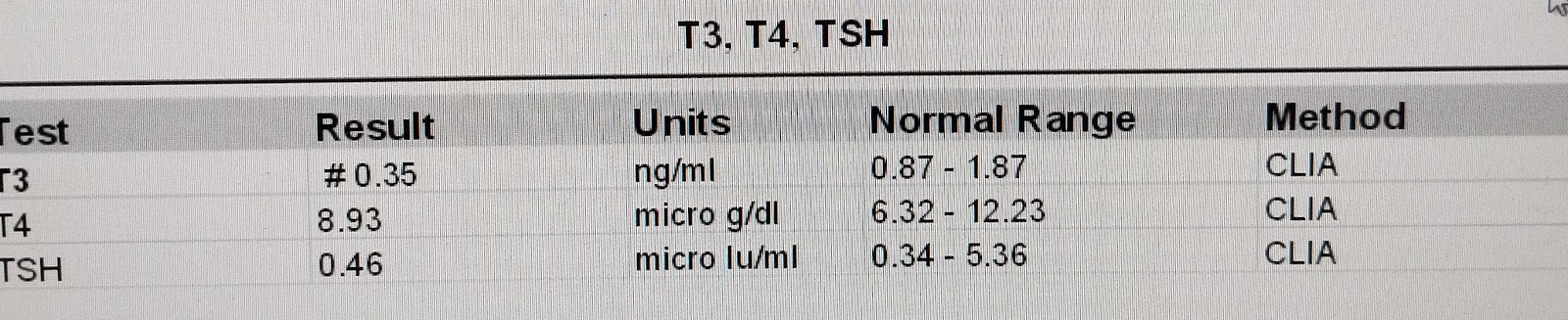
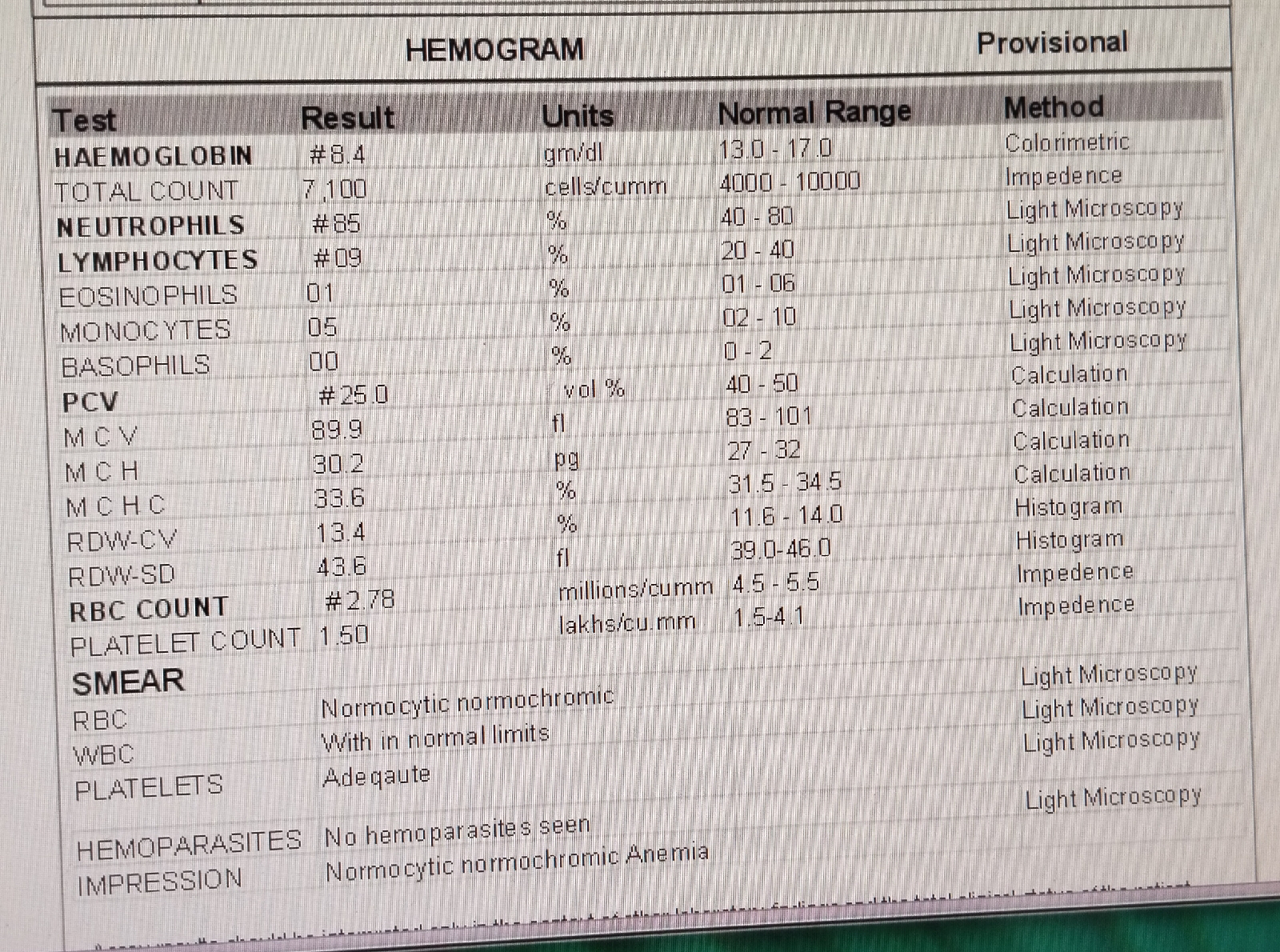
INVESTIGATIONS:




25/5/23:




26/5/23:








27/5/23:






28/5/2023:

29/5/2023:

































PROVISIONAL DIAGNOSIS
CVA WITH ACUTE ISCHEMIC STROKE (INFARCT IN RIGHT OCCIPITAL LOBE) WITH DYSELECTROLYTEMIA (RESOLVED)
WITH TYPE 1 RESPIRATORY FAILURE WITH LEFT SIDED SPONTANEOUS PNEUMOTHORAX (RESOLVING) WITH ICD INSITU IN 5TH INTERCOSTAL SPACE (29/5/23), (10/6/23)
WITH SURGICAL EMPHYSEMA
S/P TRACHEOSTOMY (24/5/23)
PYREXIA UNDER EVALUATION SECONDARY TO ? BRONCHITIS (KLEBSIELLAKLEBSIELLA ISOLATED) NOSOCOMIAL INFECTION
WITH K/C/O HTN SINCE 3 YRS.
WITH CERVICAL SPINE PLATING & REPAIR (2020)
PLAN OF CARE
1.SOFT DIET
2.IV FLUIDS NS, RL @ 50 ML/HR
3.INJ.MAGNEX FORTE 1.5G IV BD
4.TAB. CINOD 10MG PO/BD
5.TAB.MET-XL 25MG PO/OD
6.TAB.PCM 650 MG PO/TID
7.ET TUBE SUCTIONING 2ND HOURLY
8.TEPID SPONGING
9.BEDSORE DRESSING DAILY
10.POSITION CHANGE 2ND HOURLY
11.MONITOR VITALS



Comments
Post a Comment